Madison Patrick is a sociology and public health major and a 2024-25 Hackworth Fellow with the Markkula Center for Applied Ethics. Views are her own.
Despite the invaluable contribution of medical advancement to reducing maternal and fetal mortality rates, we must acknowledge the extent to which natural birthing and recovery capabilities are being undermined by efficiency-based health care practices. Research suggests that U.S. health care institutions are imposing harmful birthing practices on laboring mothers through premature or altogether unnecessary medical interventions, compromising bodily autonomy and threatening the efficacy of informed consent practices.
One of the most notable concerns is the drastic increase in cesarean delivery rates among U.S. hospitals, which research suggests has failed to improve overall maternal or neonatal outcomes, despite being developed as a resource for high-risk pregnancies and emergent delivery abnormalities (Schauer et. al). Rather, their excessive application in instances where intervention is not medically necessary has served as a detriment to this vulnerable population, increasing morbidity rates and the likelihood of complications during postpartum recovery.
Exacerbated risk factors include infection, hemorrhaging, and severe placental abnormalities alongside the substantially decreased possibility of vaginal deliveries for future births (Schauer et. al). Furthermore, this type of interference in the natural birthing process is deemed as an “emergency surgery” by medical institutions, which can levy unexpected and excessive financial burdens onto new parents, disproportionately affecting marginalized communities without health insurance and contributing to the severity of our nation's health care debt. In light of this, this paper will assess the context and evidence regarding the over medicalization of childbirth, respond to reasonable objections, and introduce a case study of personal significance to frame an ethical analysis of medical intervention practices for labor and delivery in the United States.
Evidence-Based Research on Overmedicalization
As modern medicine continues to develop, so does the reliance of physicians on intervention strategies that are now becoming routine even in standard hospital births. These include but are not limited to foley balloon inductions, intravenous infusions, oxytocin during labor, epidural analgesia, and surgical delivery through cesarean sections (Johanson et. al, 2002). A study conducted by field experts on increased obstetric intervention in birthing further suggests that inductions, epidurals, and other forms of labor augmentation increase the risk of needing an episiotomy or cesarean section during birth which gravely contributes to traumatic delivery experiences, threatens postpartum recovery, and increases the risks of complications for subsequent births (Tracy and Tracy 2004).
Financial and Social Costs of Overmedicalization
Furthermore, findings from a study focused on the association between childbirth and medical debt suggest that postpartum women have a 48% increased likelihood of facing medical debt, with similar statistics being recorded when accounting for differences in health care coverage between the public and private spheres (Cahn 2023). As anticipated, increased out-of-pocket expenses are directly associated with the surgical billing for cesarean deliveries, though the necessity of this intervention is, in many cases, subject to the discretion of the primary physician and can vary per the status and administrative goals of each medical facility.
The dire implications of this reality can be seen in a meta-analysis, which revealed that one in every three women in a fifteen-year period had been subjected to c-sections despite many of the medical justifications having been recorded as “unquantifiable ‘subjective indignations’ of fetal distress in labor” (Cooke 2020). This subjectivity is precisely why we must thoroughly consider ethical concerns in the labor and delivery process, giving particular attention to bodily autonomy, the power imbalance between patients and physicians, and the true nature of informed consent.
The Ethics of Informed Consent in Labor and Delivery
Informed consent is one of the cornerstones of ethical medical practice, intended to preserve patient autonomy, foster trust, and ensure that medical intervention is not performed under false pretenses or through coercion. Yet, in labor and delivery, this principle is frequently diluted, distorted, or altogether dismissed. The ethical complexity of childbirth, which is inevitably intensified by high-stakes decision-making, time sensitivity, and the emotional and physical demands of labor, does not excuse the undermining of informed consent. Rather, it demands an even greater commitment to uphold it and maintain strong ethical guidelines.
At its core, informed consent is defined as “an ethical ideal in which physicians are obligated to inform patients about possible medical interventions and to respect their choices regarding them” (Vaughn 2020). In line with this, four foundational conditions are established for valid consent: patient competence, adequate disclosure of information, patient comprehension, and voluntary decision-making free from coercion. These criteria, though straightforward in theory, often invite subjectivity in practice, especially during childbirth, which is notably variable and difficult to plan for.
The Role of Comprehensive Disclosure
The first and perhaps most fundamental element is comprehensive disclosure, which is often lacking in maternity care, falling prey to institutional norms and an expectation of deferral to the physician's expertise. Ideally, full disclosure would entail a comprehensive presentation of the patient’s condition, all reasonable treatment options (including the choice to decline treatment), and the risks and benefits associated with each, free of the physician's personal bias. Yet, studies show that adequate disclosure is routinely neglected in labor and delivery, which may be indicative of institutional standards of avoidance for the efficiency delays caused by patients’ prolonged deliberation. For instance, “Consent forms for pain medications, to mention just one example, often do not describe the labor-altering effects and side effects of these drugs” (Lowe 2004, cited in Tores & De Vries 2009). This omission not only undermines informed consent but also reinforces the problematic belief that women are incapable of participating in meaningful decision-making once labor has begun, and that deviations from their birth plans should be primarily at the discretion of the physician.
Defining Competence in the Delivery Room
The second condition, competence, is another matter of dire ethical importance. Competence is generally presumed unless cognitive impairments or conditions such as dementia, psychosis, or intoxication interfere with decision-making. However, in labor, competence is often wrongly presumed to be diminished. The physiological intensity of childbirth, including pain, exhaustion, and fear, is at times cited to justify overriding the woman’s expressed wishes and even active objections. Irrespective of the inevitable toll that childbirth takes on one’s body and mind, the ability to provide consent to intervention should be assessed in the same manner as any other patient enduring stressful conditions (Flanigan 2016).
All the more, laboring mothers can be argued to have better preparation than an average patient to comprehend their treatment options and make an informed decision due to the added element of prenatal research and pregnancy monitoring. In line with this, the discernment of competence must be based on the capacity of the patient to meet the conditions of an informed choice, not on whether her decision aligns with medical recommendations. For the concept of informed consent to retain its validity in the field of medicine, patients must be afforded genuine protections that allow them to diverge from the recommendations of their physician without being shamed, ignored, or deemed incompetent.
The True Nature of Voluntary Consent
This brings us to the most commonly violated aspect of informed consent in labor: voluntariness. In the clinical setting, especially in obstetrics, power asymmetries between physicians and patients are exacerbated. Laboring women are acutely vulnerable and navigating a deeply emotional and painful experience with limited time and immense pressure.
Physicians, armed with technical knowledge and institutional authority, may unintentionally wield this power in ways that diminish patient agency and enhance social stigma regarding maternal judgment. Well-intentioned providers may urge interventions out of concern for fetal well-being, but when such recommendations are delivered as ultimatums or with manipulative framing, they can amount to coercion. It is crucial, then, to acknowledge that just as we have a reasonable expectation that a physician will act in the best interest of their patient, we can similarly presume that patients will generally avoid severe risks to preserve their life and well-being, as well as that of their child.
While the interventions of physicians may be benevolently motivated, they can ultimately manifest as obstetric violence rooted in paternalism, a form of subordination guided by the belief of acting in a patient’s best interest. In counteracting this approach, we must recognize that health is only one of many values, and the ultimate priorities of the patient may not always align with the physician's, but must be protected nonetheless. Flanigan highlights this reality, noting, “Women's interests in making decisions about labor and delivery are not only informed by their medical needs, but also by their values, tolerance for risk and pain, and how they weigh health against other elements of well-being (2016). Furthermore, a patient may prioritize their cultural and spiritual beliefs or laboring techniques inspired by alternative medicine above clinical efficiency, and marginal reductions in statistical risk, which is entirely valid.
While subject to change when a patient is provided with new information, birth plans are often a strong indicator of a mother’s values and intentions, and yet are frequently undermined as a mere outline of preferences. This forces them to function then as defensive documents and “weapons in an adversarial struggle,” as Tores and De Vries (2009) describe, referencing the work of Lothian and Shaw. This characterization suggests that the very need for such documentation is indicative of the deep mistrust in the provider-patient relationship. Birth plans represent a preemptive assertion of genuine consent and autonomy in a space where many women fear they will be silenced, coerced, or sidelined.
The Ethics of Autonomy in Labor and Delivery
Obstetrics is one of the most ethically complex fields in health care, where a mother’s autonomy is too often compromised by institutional norms and pressures, and professional authority expressed as paternalism. Despite a global emphasis on human rights in health care, laboring women continue to experience concerning violations of their dignity, privacy, and autonomy both physically and psychologically. Health care providers often face the difficult task of balancing medical judgment with respect for patient autonomy. They may believe that advocating for certain interventions is in the patient’s or fetus's best interest, and in many cases, their intentions are not malicious. However, exerting pressure, even subtly, can quickly cross ethical boundaries.
An article published in The Independent notes, “Pressure, manipulation, and coercion are not uncommon in the delivery room,” and while physicians may feel it is their duty to recommend certain actions, the ultimate decision lies with the patient and should be respected as such (Grant 2017). Unfortunately, there remains a widespread misconception that accepting the care of a physician at a hospital and even just the broader act of being in labor diminishes one’s decision-making authority. This misunderstanding is perpetuated by both cultural signaling and clinical environments where defensive medical practices and associated coercion, even if unintentional, are deeply ingrained.
The Capacity of Laboring Mother’s for Autonomous Decision Making
The American Sociological Association's principles on respect for persons emphasize the right of individuals to make autonomous decisions about their own bodies, with special care taken for those with diminished capacity (Tores & De Vries 2009). Evidence suggests that laboring women should remain fully equipped with their autonomy, as targeted tests measuring the relationship between labor pain and comprehension suggested no reduction in decision-making capacity (Jackson et al. 2000). Nonetheless, ethical tension is exacerbated by concerns for fetal well-being, which may at times seem to conflict with maternal autonomy. While this is a valid point of consideration, and patients and physicians alike have a strong ethical obligation to consider the health of unborn children, the ultimate legal and moral authority still lies with the women in upholding bodily autonomy.
Just as with any competent patient, a physician's expert advice is a significant guiding factor, but unwanted interventions that threaten the rights of the patient are not warranted. As Flanigan argues, “Though women in hospital settings are vulnerable to social pressure and coercive influences, the remedy for this vulnerability is to treat them as competent and to fully inform them about their treatment options, not to render them unable to consent and then to justify breaches of informed consent requirements on other grounds” (Flanigan 2016).
Respecting autonomy in childbirth demands that clinicians see their patients not as passive recipients of care, but as autonomous moral agents capable of weighing their own risks, priorities, and dignity. To promote anything less is to prioritize control over care, and to threaten the fundamental boundaries of bodily and psychological autonomy.
Personal Case Study
In her first three experiences with childbirth, my maternal grandmother, Claudia Lowrey, navigated the landscape of maternal health care in anticipation of a typical hospital birth with minimal intervention. Receiving routine prenatal care and having pregnancies relatively free of complications, she held a reasonable expectation of receiving the appropriate guidance and respect for her autonomy during her labor and delivery. Contrary to this, in one delivery, she recalls engaging in routine breathing strategies during labor, and without consent or explanation, being administered the sedative, Valium, through her IV to address her assumed hyperventilation. Ultimately, the medication served only to numb her body and prevented her from fully engaging throughout the pushing phase of her delivery, without mitigating any of the pain or worry she was experiencing.
Claudia hoped that this lack of informed consent or respect for her bodily autonomy was an exception, rather than a typical occurrence in maternal care, but upon the delivery of her next child at the hospital, she faced similar challenges. In this instance, after giving birth, she was hemorrhaging blood and the doctors followed the standard practice of packing her vaginal canal with gauze. While this was a reasonable course of action, the nurses on staff failed to inform Claudia and even failed to mark this occurrence on her medical chart, causing her to be sent home without their removal. The fear that overwhelmed Claudia upon returning home and having the blood-soaked gauze that she wasn’t previously aware of, now falling out of her body, is something that no patient should have to experience. Fortunately, she was rushed to the hospital for postpartum care before the gauze led to an infection and further threatened her health.
These traumatizing experiences of being largely disregarded and uninformed about the medical interventions taking place during her delivery left a deep impression that ultimately informed her decision to give birth to her third child at home. With the support of midwives, who involved her at every stage of the birthing process, Claudia delivered a healthy baby boy in the comfort of her own home and felt connected to herself and her child in a way that she never had with her previous hospital experiences. A few years later, she found that she was pregnant once again, and given the challenges that she had faced with medical intervention previously and the drastic difference in the experience of her first natural home birth, Claudia elected to have another midwife-guided home birth. Even after finding out that she would be having twins and consulting her prenatal care team about the increased risks of a double birth, she stood by her decision to protect her autonomy and prepared as best as she could for the experience to come.
Empowered and determined to defend herself and her children, Claudia delivered two healthy, six and seven-pound baby girls at home with the support of her midwives and husband. As she lay with relief and prepared to birth the placenta, her care team was taken aback in disbelief–a third child was still in her womb and ready to be delivered! Utterly surprised, she gave birth to the final baby of her newfound triplets and was blessed with another girl in perfect health.
Knowing the high frequency of cesarean sections encouraged by physicians even in single births, she likely would have been pressured into an interventional delivery route to mitigate potential risks and would have sacrificed her natural birthing experience with her triplets. While Claudia’s story was certainly unique, it symbolizes the extent to which women are fighting to protect themselves and their birthing experiences, amidst having their informed consent undermined, their competency underestimated, and their bodily autonomy threatened in hospital settings.
A newspaper clipping featuring an article about Claudia and Steve Lowrey and their triplet daughters Rebecca, Jessica, and Rachel. Article by Tina May, Sun Staff Writer, and the photo by Sun staff photographer Hal Stoelzle.
Lowrey Infants: Triplets Rebecca, Jessica, and Rachael laying side by side swaddled in baby blankets. Photo by "The San Bernardino Sun" photographer Hal Stoelzle.
Addressing Opposition
While the immense value of modern medical advances and formally trained obstetricians can not be understated, it is still crucial to acknowledge that any intervention used in excess must be regulated to better protect our vulnerable populations. By setting functional standards for physicians to utilize in their discernment of medical intervention necessity, we can reduce the prevalence of overmedicalization and subsequent complications that have defined the anecdotal narratives surrounding our nation’s culture of obstructive hospital birthing practices.
Furthermore, when invasive actions are not immediately taken by physicians in response to labor and delivery complications, parents are given the autonomy to explore alternative resolutions through the process of informed consent. This can lead to decreases in the alienation frequently cited by mothers, while also shifting a degree of liability onto the patients in accordance with the extent of risk and nature of the intervention that they are willing to bear. Crucial to this process is the support of teams of providers who can assist in the education and decision-making process for new parents.
How Health Care Knowledge and Support Diverge from Overmedicalization
First, it must be acknowledged that extenuating societal conditions beyond the scope of Western medical capabilities have contributed to decreases in maternal and fetal mortality and morbidity. As is referenced in a clinical research source, health improvements are reflective of broader developments in areas such as “disease control, smaller family sizes, and higher standards of living [and] improved diet” (Johanson et. al 2002). Though I am in no way suggesting that medical interventions are not to be valued and utilized in hospital birthing procedures when appropriate, I must emphasize that my position is against overmedicalization, which can unnecessarily transform natural experiences of familial expansion into traumatic experiences of surgery and invasive procedures.
Citing the ability of providers to address the subsequent health detriments of medical intervention in the delivery process does not negate the reality that some may have been avoidable altogether, were regulations to be instituted on physician discretion. This is all to suggest that physicians’ education, training, and experience are not intended to be undermined by the proposed regulatory standards. Rather, the application of their abilities will be enhanced in the process of recovering patient-centered birthing practices to uplift patients’ decision making instead of oppressing them when they have so much at stake.
Changing our Culture of Health Care & Defensive Medicine Practices
Health care culture in the U.S. is known for prioritizing the success and discretion of individual physicians as utility players, as opposed to incorporating providers with varying expertise as a network of support to ensure the quality of care for patients. Not only are obstetricians constantly faced with high-intensity circumstances, but even momentary hesitations in providing care may be at the expense of a mother's or child’s life.
This is further exacerbated by the fact that maternal vital signs, physiological symptomatology, and laboratory values are subjected to substantial variations from standard care guidelines, which pose an increased risk for unaddressed clinical deterioration at the liability of the supervising physician (Shauer et. al, 2024). Understandably, being held accountable as a physician for instances of unnecessary intervention in the labor and delivery process is far less threatening to one’s career, reputation, and financial standing when compared to malpractice claims for maternal or fetal mortality (Johanson et. al, 2002).
This often manifests as defensive care behaviors, which include “actions taken by physicians that lack medical necessity [as well as] abstaining from high-risk procedures that are medically warranted and could benefit the patient,” with an underlying objective of avoiding adverse consequences and liability (Eftekhari et. al, 2023). Objections surrounding malpractice liability can be drastically resolved when a team of educated individuals collaborates in their assessment of possible emergent complications to aid parents in understanding their options and utilizing medical intervention strategies when deemed necessary.
The Patient Safety Network references the AHRQ Safety Program for Perinatal Care, which identifies strategies for improving maternal safety built upon the following pillars: communication and functionality among teams of care providers, clinical simulations for experiential training purposes, and perinatal safety strategies such as “safe electronic fetal monitoring, rapid response, [and] medication administration,” to address complications before they require invasive interventions (Shauer et. al, 2024). Regulatory standards implemented for hospital birthing practices can be built upon these very principles, dismantling the culture of exclusivity through balanced responsibility among teams of providers, and ultimately reducing the liability concerns that incite fear-driven intervention.
Addressing Physician Shortages and Institutional Pressure
Foremost, while I recognize that this may be an idealized claim to make, quality of care can not be sacrificed for patient quantity. A shortage of maternity health care providers amidst increasing demand should not attempt to be reconciled with efficiency-based practices at the expense of the safety and experiences of birthing mothers. Rather, investments must be made to incentivize the specialization of health care providers in obstetric services, similar to the dilemma being faced with shortages of mental health providers. This is particularly critical for the geographical regions labeled as “Maternity Care Deserts” in the figure below, encompassing 36% of counties nationwide that are absent of obstetric providers and hospitals offering obstetric care (March of Dimes 2022).
This research provides further support for changes in the fiscal domain of our health care system to financially support the educational training, residency, and professional application of medical students to the field of obstetrics in exchange for their geographical commitment to areas of severe maternity provider shortages. In response to concerns of institutional pressure, I would argue that instating regulations on intervention reliance will shift the burden from individual physicians to the broader health care facilities as they acclimate to new standards of care that increase an overarching accountability for the quality of birthing experiences.
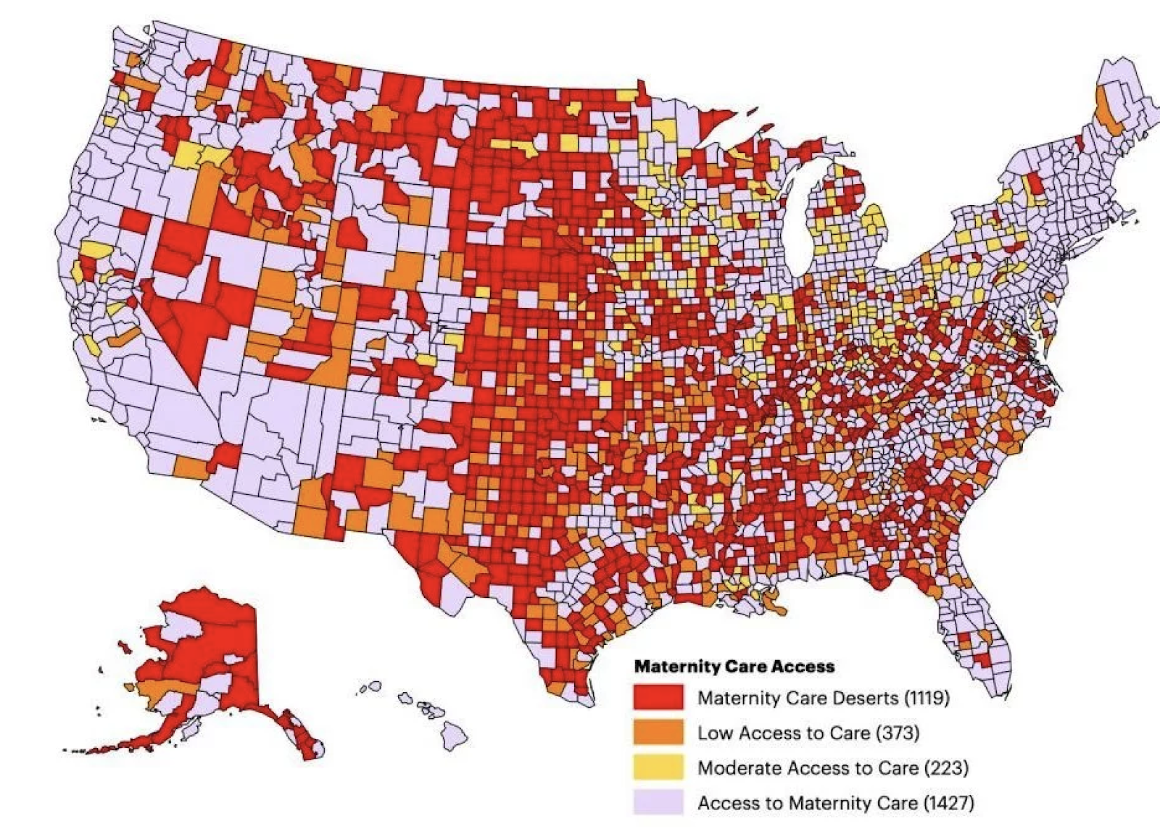 Maternity Care Deserts, 2020
Maternity Care Deserts, 2020
Source: U.S. Health Resources and Services Administration, Area Health Resources Files, 2021
Position Reassertion and Ethical Implications for Marginalized Groups
The continued reliance of obstetric physicians on intervention procedures that create further maternal and fetal risk is indicative of the underlying failures of a health care system that prioritizes institutional efficiency, financial incentive, and physician convenience above the quality of care for vulnerable populations. Those in opposition to regulating overmedicalization practices fail to recognize that childbearing is a unique and multi-faceted experience in which medical intervention can, in many ways, serve as a detriment unless emergent need is indicated.
This issue further invokes the consideration of how increased costs for “emergency” interventions during the labor and delivery process are contributing to our nation's health care death rate and are discouraging mothers from seeking further support from their health care providers during postpartum recovery.
Anecdotal experiences suggest that unanticipated medical intervention during childbirth contributes to feelings of alienation and a lack of control for new mothers (Williams and Umberson 1999). Additionally, the cost increases associated with interventions categorized as emergent have further implications for low-income and uninsured families, with research suggesting wide ranges of “adverse effects on the growth, development, health outcomes, and food security of children” (Cahn 2023). Combatting individualistic cultures in health care decision-making and reinstating the importance of patient autonomy, alternative support measures, and informed consent are crucial to reducing the unnecessary overmedication of childbirth.
Moving forward, we must recognize that childbirth is not a problem to be solved, nor a liability to be managed. It is an intimate, human experience that demands the highest standard of ethical care. If we truly value autonomy in medicine, we must honor it even, and especially, when the stakes are high.
References
Cahn, Julia, Aditi Sundaram, Rishi Balachandar, Allison Berg, Alex Birnbaum, Samuel Hastings, Max Makansi, Elina Romano, Arianne Majidi, David McCormick, and Adam Gaffney. 2023. “The Association of Childbirth with Medical Debt in the USA, 2019–2020.” Journal of General Internal Medicine 38(10):2340–2346.
Cooke, Jennifer. 2020. “Intimate Odyssey: Modern Motherhood and the Birth Narrative.” Virginia Quarterly Review 96(4):26–37.
Eftekhari, M. H., Parsapoor, A., Ahmadi, A., Yavari, N., Larijani, B., & Shamsi Gooshki, E. (2023). Exploring defensive medicine: Examples, underlying and contextual factors, and potential strategies – A qualitative study. BMC Medical Ethics, 24, Article 82.Johanson, Richard, Mary Newburn, anJohanson, Richard, Mary Newburn, an
Flanigan, Jessica. 2016. “Obstetric Autonomy and Informed Consent.” Ethical Theory and Moral Practice 19(1):225–244.
Jackson, A., D. Henry, N. Avery, and J. Taylor. 2000. “Informed Consent for Labour Epidurals: What Labouring Women Want to Know.” Canadian Journal of Anaesthesia 47(11):1068–1073.
Johanson, Richard, Mary Newburn, and Alison Macfarlane. 2002. “Has the Medicalisation of Childbirth Gone Too Far?” BMJ (Clinical Research Edition) 324(7342):892–895.
March of Dimes. 2022. Maternity Care Deserts Report.
Schauer, Madeline, Alison Nichols, and Audrey Lyndon. 2024. “Maternal Safety.” Agency for Healthcare Research and Quality Patient Safety Network.
Torres, Jennifer M., and Raymond G. De Vries. 2009. “Birthing Ethics: What Mothers, Families, Childbirth Educators, Nurses, and Physicians Should Know about the Ethics of Childbirth.” The Journal of Perinatal Education 18(1):12–24.
Tracy, Sally K., and Michael B. Tracy. 2004. “Costing the Cascade: Estimating the Cost of Increased Obstetric Intervention in Childbirth Using Population Data.” BJOG: An International Journal of Obstetrics and Gynaecology 110(8):717–724.
Vaughn, Lewis. 2020. Bioethics: Principles, Issues, and Cases. 4th ed. New York: Oxford University Press.