1. Study Description
This study investigates the use of biofeedback mechanisms to control physiological signals, such as heart rate variability (HRV) and breathing rate, in response to stressful situations. Using a virtual reality (VR) setup, participants are trained to regulate their physiological responses in a non-stressful environment, followed by a session in a stress-inducing VR environment where they must apply these techniques. The goal of the study is to assess whether biofeedback training can help individuals manage their physiological responses to stress in real-time. The broader objective is to explore the applicability of biofeedback training for managing stress and anxiety in real-world scenarios, with a potential focus on clinical applications such as anxiety management and mental health therapy.
Additional background on the technologies in this study may be found in the Appendix.
Part 1: Biofeedback Training in a Non-Stressful Environment
In the first phase of the study, participants engage with a VR game designed to provide a calming and non-stressful environment. During this session, participants are taught biofeedback techniques, specifically focusing on controlling their heart rate and breathing.
Participants wear physiological sensors that measure heart rate variability and breathing patterns in real-time. They receive visual feedback within the VR game, helping them learn how to adjust their breathing to control physiological stress markers. The objective of this phase is to teach participants to regulate their physiological responses in a calm setting, before moving on to more stressful scenarios.
Part 2: Application of Biofeedback in a Stress-Inducing Environment
In the second phase, participants are introduced to a VR game that simulates a stress-inducing scenario. This environment is designed to mimic a high-stress situation, similar to a horror movie, where participants are required to apply the biofeedback techniques they learned in the first phase. Participants must regulate their physiological responses in real-time to avoid "detection" by in-game elements. For example, heart rate control may be required to prevent virtual enemies from noticing the participant’s presence. This phase assesses whether the biofeedback techniques taught in the non-stressful environment can be effectively applied in real-time during stressful situations. The data collected during this phase, such as changes in heart rate variability and breathing patterns, is compared to baseline readings taken during the non-stressful phase to evaluate the effectiveness of the biofeedback training.
Ethical Challenges
The open-ended query for this case study seeks to explore the potential risks associated with biofeedback psychology research, including safety protocols, user experiences, and data management.
- How does this research pose ethical challenges, particularly in terms of participant consent and psychological safety?
- Where do you suspect there are issues with the data collected in the study?
Collect your group's thoughts in the Open Inquiry Notes
2. Technical Description
The technical setup involved the integration of various physiological sensors and a VR system to provide real-time feedback to participants. Key components of the technical setup included:
- Pulse Sensors: These sensors measured heart rate and heart rate variability, providing critical feedback for assessing participant stress levels.
- Respiratory Bands: Used to measure breathing rate, these bands played a key role in the breath-control biofeedback mechanism.
- Skin Conductance Sensors: These measured the electrical conductance of the participant’s skin, an indicator of stress and emotional arousal.
- VR System: A high-resolution VR headset provided immersive experiences to induce stress, while simultaneously allowing for real-time feedback on physiological metrics. Challenges during the study included ensuring that the VR system did not interfere with the sensors and that participants were comfortable wearing the equipment for prolonged periods. Careful pre-testing and calibration of all devices were critical to the study's success.
Mental Health Data
Participants completed surveys on anxiety, depression, interoception, and gaming history. These were used as covariates to the physiological metrics.
Participant Activities
Participants completed the surveys first. Then they were trained on the target breathing pattern. The VR sessions were a breathwork and a stress-induction, which were each 10- minutes. The participants rated their stress state following each condition.

Figure 1. In the training session, participants' HR trace was fed back to them (cyan trace in the prow of the boat), and they also received both written and verbal instructions on the breath regimen. Further ambient sounds of the water were presented to encourage relaxation.
(Image: View from a rowboat onto a calm open water with cloudy orange sky. Overlay of pulse waveform and text of “this boast is being driven by your own biometrics.” Source: https://doi.org/10.1111/psyp.14705)
Safety During Stress-Inducing Sessions
Prior to the conduct of this study, stress scenes were screened by pilot group to rate intensity on a 10-point scale. Only scenes rated 7 and below were included in the full study as they were sufficient to induce a stress responses and were not at an intensity that produced extreme stress or fear in typical adults.

Figure 2. In this still, the participant is looking down and can see a representation of their body including the attachment of the pulse device to their right index finger. The stress monitor (top right) was experienced as being fixed to their headset so that it was always in their field of view no matter where they looked. In the image, their stress index is within the “safe zone” (with the indicator to the left of the display and the green light on). When aroused it could move to the “danger” or “death” zones.
(Image: View of hands and legs with a data monitor to the right and a skull at the feet. Source: https://doi.org/10.1111/psyp.14705)
Technical Analysis
- How does the study design balance evocation of a stress response and participant well-being?
- Does the use of biofeedback, the translation of physiological data into an interactive component for the participant, alter the impact of the data collection? This in contrast to offline analysis or researcher monitoring of biodata.
Collect your group's thoughts on the Technical Analysis Notes
3. Risk Analysis
The study was reviewed and approved by the Institutional Review Board (IRB) of the medical school as a biomedical research protocol. The principal investigator is a psychiatrist. Calibration of the stress-induction intensity was requested prior to the initiation of the full study.
Informed Consent
Participants were provided with an informed consent document with the required section. Each topic was in plain language with a question, as in an FAQ. For example, "Will I be paid for my time?" (The compensation was 1.5 hours at minimum wage.)
The consent acknowledgement was done per item as shown below. It separately highlights the nature of the content, data privacy mitigation efforts, and permission for future use. Participants could selectively consent to public use of data.
|
# |
Consent Acknowledgement |
√ |
|---|---|---|
|
1. |
I confirm that I have read, understood and accept the conditions in the information sheet, version 1 dated Dec 2021, for the above study, and I have had the opportunity to ask questions and have them answered. |
|
|
2. |
I understand that this study involves a stressful game equivalent to a R15** horror film |
|
|
3. |
I understand that my personal information, which links me to the research data, will remain confidential and that all efforts will be made to ensure I cannot be identified (except as might be required by law). |
|
|
4. |
I agree that data gathered in this study may be stored anonymously and securely, and may be used for future research. |
|
|
5. |
I understand that my participation is voluntary and that I am free to withdraw at any time without giving a reason. |
|
|
6. |
I consent for my fully anonymized data to be shared in a publicly accessible scientific repository such that other researchers may reuse said anonymous data as they see fit. |
|
|
7. |
I agree to take part in this study. |
*Source: Paul Fletcher, University of Cambridge
**Suitable only for those aged 15 and over
Data Privacy
All collected physiological data, such as heart rate and breathing patterns, were anonymized to ensure participant confidentiality. Data was securely stored on encrypted, password-protected servers, and access was limited to authorized personnel.
Participants were asked for explicit consent before their data could be used for future research beyond the scope of this study. The data will be stored for 10 years. Data sharing would occur with only non-indentifiable data types.
Risk Assessment
- What are the key risks to participant safety in this study? How did the review process address these risks?
- Was the informed consent as described sufficient to educate the participants prior to enrolling in the study? How?
Collect your group's thoughts on the Risk Assessment Notes
4. Conclusion
The study yielded significant insights into the use of biofeedback for managing stress in real-time. Participants who followed the breath-control techniques during the stress-inducing VR session showed improved heart rate variability, suggesting that biofeedback can be effective for short-term stress management.
These findings have broader implications for therapeutic practices. Biofeedback may be a valuable tool in clinical settings for treating conditions such as anxiety and PTSD, as it allows patients to develop greater control over their physiological stress responses. Future studies should explore the long-term effects of biofeedback training and its potential integration into therapeutic programs.
To balance risk with research objectives, a framing by stakeholder is helpful. Who is responsible for managing the type of risk? The following table summarizes the main risk categories and the mitigation strategies applied in the study. Please review to inform the discussion.
Risk Categories, Stakeholders, and Mitigation Strategies
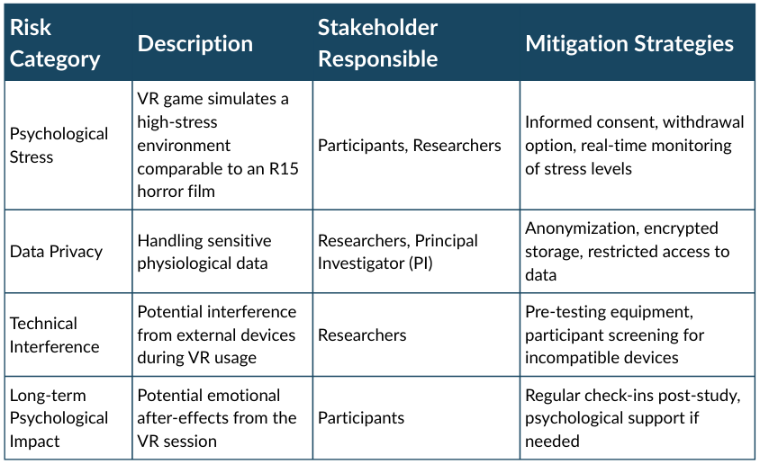
(Image: Table with column headers Risk Category, Description, Stakeholder Responsible, Mitigation Strategies with respective lists of Psychological Stress, Data Privacy, Technical Interference, Long-term Psychological Impact, then VR game simulates a high-stress environment comparable to an R15 horror film, Handling sensitive physiological data, Potential interference from external devices during VR usage, Potential emotional after-effects from the VR session, then Participants/Researchers, Researchers/Principal Investigator (PI), Researchers, Participants, then "Informed consent, withdrawal option, real-time monitoring of stress levels", "Anonymization, encrypted storage, restricted access to data", "Pre-testing equipment, participant screening for incompatible devices", "Regular check-ins post-study, psychological support if needed". Source: Scott, Chaudhary, Bagade, 2024.)
Mitigation Strategy
- What did the researchers and IRB do to protect participants from undue risk? Would you recommend additional steps or a different approach?
- Do you believe the psychological risks are greater in a virtual reality environment compared to a flat screen? If so, what do you think the boundary conditions should be?
Collect your group's thoughts on the Mitigation Strategy Notes
Acknowledgments
The research team would like to acknowledge the Cambridge University research group that shared their study materials and consulted for this project.
Appendix
Virtual Reality and Embodiment
"The sense of embodiment refers to the sensations of being inside, having, and controlling a body. In virtual reality, it is possible to substitute a person’s body with a virtual body, referred to as an avatar. Modulations of the sense of embodiment through modifications of this avatar have perceptual and behavioural consequences on users that can influence the way users interact with the virtual environment." (Guy et al., 2023)
Effective embodiment and the sense of presence in VR induces the illusion that the experience is happening to your own body. This is distinct from watching or observing a character in a game or movie that one identifies with or empathizes with. It is more similar to the rubber hand illusion, in which a rubber hand positioned to obscure someone's real hand can produce the sensation of touch through watching the rubber hand be touched. The intensity of the experience is heightened in embodied VR (Goth et al., 2021). The embodied experience of first person view immersive interactions must consider how it will impact the participants sense of safety.
Virtual Reality and Memory
Virtual reality is commonly used for role-playing based training, such as sexual harassment training, and simulation based training, like first responder crisis scenarios. The reason for this is that the rate of learning is accelerated and the transfer of learning to real application is enhanced. These statistics imply that memory formation is more effective in VR. When studied directly, memory performance gains in VR are explained by arousal and presence, independent of the realism of the visual quality (realism) (Cadet and Chainay, 2020). Knowing this, one muse re-evaluate the nature and intensity of VR experiences for research.
Physiological Data
Measurement of "vitals" (pulse, breath, etc.) may appear innocuous. However, when analyzed in context, they reveal one's unmasked response to stimuli. These autonomic reactions to emotional shifts (like stress) are distinct from the semantic sharing of feelings and mental states ("I'm scared"). In neuropsychology research, it is considered an objective measure of emotion. Yet it may also be described as a private expression of emotion. When these data are used in research, it is important to explain to the participant that the biodata collected will represent their mental and emotional states. These data types and analytics should be treated in a manner similar to other sensitive psychological reports.
Some physiological data also has the potential to uniquely identify a person. This is possible with EKG and EEG, which were not collected in the present study. These data should be stored with the same level of security as other sensitive and identifying information.
References
[1] Daniel‐Watanabe et al., “Using a virtual reality game to train biofeedback‐based regulation under stress conditions,” Psychophysiology, vol. 62, no. 1, p. e14705, Jan. 2025, doi: 10.1111/psyp.14705.
