
Medical professional evaluating a young patient in gynecology clinic. Photo by Mariakray via Adobe Stock.
Karina Martinez is a double major in biology and neuroscience and she is a 2024-25 health care ethics intern at the Markkula Center for Applied Ethics at Santa Clara University. Views are her own.
"I learned from TV, which made me sad because it didn’t sound real."
Karla Cortez,a junior business major, was raised in a Mexican Catholic household where sex was a taboo topic.
"My mom would tell me, ‘You don’t have to wait until marriage... just be sure about who you’re with. A lot of [my friends] who I knew had religious families and who were too shy to talk about sex education with their children, thinking it might push them towards having sex in the future. They’re the ones who actually ended up having kids at a very early age."
Samantha Soto, a junior marketing major raised in a Peruvian home where conversations about sex were early and honest.
"Although you should wait for marriage, if you do it, at least do it with someone you love."
Justin Marquez, junior biology major raised in a Puerto Rican and Costa Rican Christian household.
For Hispanic adolescents like Karla and Justin, talks about sex and contraception came from the media, silence, religious influences, or for a few like Samantha, from honest conversations at home. While some parents offer guidance on navigating sexual relations, many in the Hispanic community leave adolescents searching for guidance elsewhere.
Disparities in Use and Access to Contraceptives
Adolescence, defined by the World Health Organization (WHO) as individuals aged 10–19, is a vital period for sexual health education and interventions. This chapter marks a transition from childhood dependency to adult independence. The term Hispanic is defined as “individuals from Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish cultures, regardless of racial identity.”
The disparities in contraceptive use among Hispanic adolescents significantly impact unintended pregnancy rates. Hispanic adolescents utilize contraception at nearly half the rate of white adolescents, with only 12% of Hispanic adolescents using contraception at their last intercourse compared to 24% of white adolescents. Among those using contraception, Hispanic adolescents tend to use less effective contraception methods, with only 18% using prescription contraception compared to 38% of white adolescents. As a result, Hispanic adolescents experience significantly higher pregnancy rates: 25.3 births per 1,000 adolescents, compared to 11.4 births per 1,000 non-Hispanic white adolescents. These pregnancies can lead to disruptions in educational attainment, economic status, and overall mental and physical well-being, which can also affect the next generation’s health outcomes.
Let’s [Not] Talk about Sex
In many Hispanic households, talking about sex is often shaped by familismo: a cultural value that emphasizes strong loyalty, attachment, and obligation to both immediate and extended family members, marianismo: where women are expected to be naive and virginal/pure, and machismo: where men are expected to be dominant.
Often, familismo can be a double-edged sword as it can foster support and guidance, but can also lead to discomfort and challenges in accessing adolescent sexual and reproductive health (ASRH) education and care.
Experiences like those of Karla, Samantha, and Justin are not independent. Many Hispanic parents assume adequate sex education is already covered at school. However, in rural communities, federally funded abstinence-only-until-marriage programs remain prevalent in rural schools primarily serving Hispanic adolescents. These programs often provide incomplete, misleading, or unscientific information on pregnancy prevention, HIV, and other sexually transmitted infections. In 2018, the CDC found that Hispanics/Latinos accounted for 27% of the 37,968 HIV diagnoses in the United States and dependent areas. This must be addressed as many Hispanic adolescents, particularly those living in rural communities, are not receiving adequate ASRH education.
Adolescents like Samantha describe benefitting from having inviting, honest conversations about sexual relations at home. Her mother, Rosa Soto, broke the generational silence because she “did not want [her daughters] to be afraid or unprepared,” as she once was. Parental comfort in discussing sexual health is one of the most powerful facilitators for contraceptive use among Hispanic adolescents.
Individual, interpersonal, and health care provider factors all facilitate access to contraception. These include parental comfort when talking about sexual health, supportive friends with positive contraceptive experiences, clear future plans, and health care providers who prioritize privacy, communication, and respect.
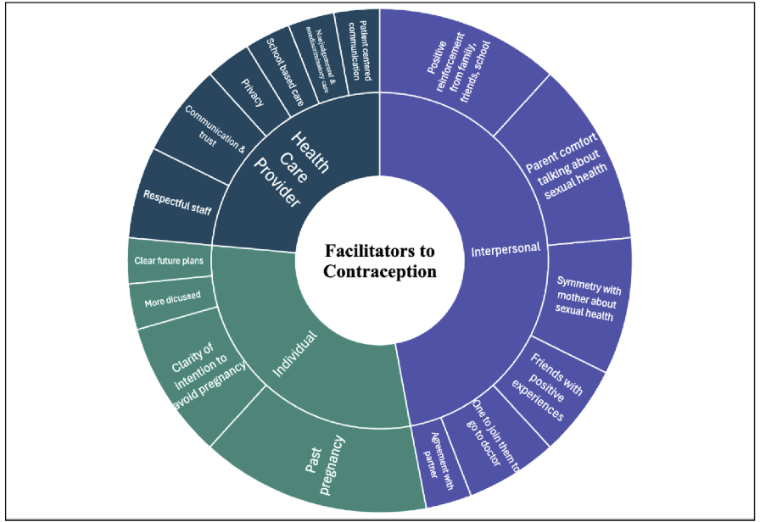 Figure 1. Facilitators to Contraception. The central themes include related subthemes, and the size of each section is proportional to the frequency with which each theme was mentioned across 16 studies. © 2024 Batek et al, National Library of Medicine, CC by 4.0.
Figure 1. Facilitators to Contraception. The central themes include related subthemes, and the size of each section is proportional to the frequency with which each theme was mentioned across 16 studies. © 2024 Batek et al, National Library of Medicine, CC by 4.0.
However, these facilitators are often met with multiple barriers. For instance, individual barriers include factors such as dislike of contraception, misconceptions, or pregnancy risk perceptions. Interpersonal factors, such as familismo, fear of family dishonor, or prohibition of birth control, can discourage contraceptive use. Structural barriers include cultural and religious beliefs, geographical location, financial limitations, and language barriers, which can further complicate access. For example, Hispanic families are more likely to be uninsured. In 2023, 63% of uninsured adults said coverage was too expensive, and uninsured individuals were more likely to delay or forgo care.
Within health care settings, Hispanic adolescents report experiencing discrimination, poor communication, and mistrust of health care providers. This further discourages them from accessing contraceptives as there is no support offered.
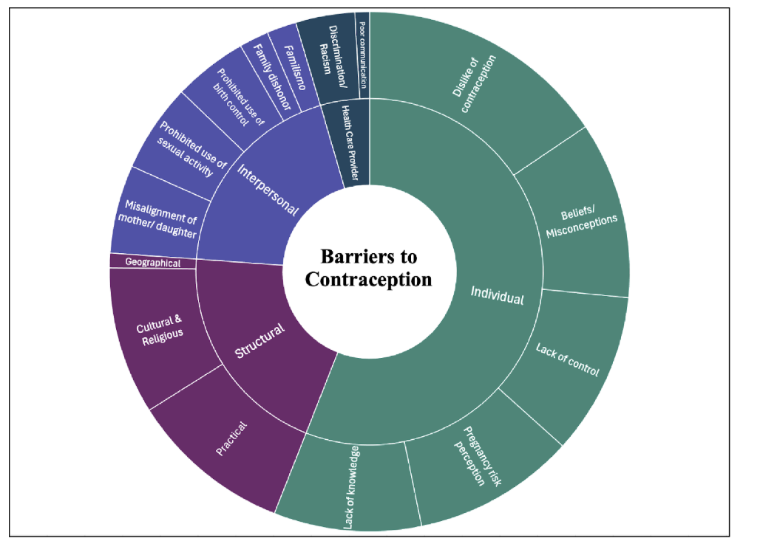 Figure 2. Barriers to Contraception. The central themes include related subthemes, and the size of each section is proportional to the frequency with which each theme was mentioned across 16 studies. © 2024 Batek et al, National Library of Medicine, CC by 4.0.
Figure 2. Barriers to Contraception. The central themes include related subthemes, and the size of each section is proportional to the frequency with which each theme was mentioned across 16 studies. © 2024 Batek et al, National Library of Medicine, CC by 4.0.
Sex Health Education in Schools
The National Sex Education Standards (NSES) were developed in 2012 and updated in 2020 to provide school districts with age-appropriate guidance on sexual health education. Many Hispanic adolescents report that their school’s sex education classes are minimal and focus on general health or abstinence. A lack of comprehensive sex education often leads adolescents to turn to inaccurate sources such as the Internet or the media. Meanwhile, comprehensive sex education shows an increase in healthy relationships, familial communication skills, social-emotional learning, and media literacy.
Reproductive Justice
Reproductive justice emphasizes that all people have the right to bodily autonomy, to have children, not have children, and to parent their children in safe communities. Applying this framework means recognizing the impact systemic barriers (such as racism, poverty, lack of health care) and misinformation have on the decisions Hispanic adolescents make when it comes to contraceptive use.
Therefore, Obstetricians-Gynecologists (OB-GYNs) should provide patient-centered contraceptive counseling that prioritizes the patient’s own values and cultural needs. This also requires that providers recognize counselor biases, historical and ongoing reproductive mistreatment, and structural inequities that Hispanic adolescents face that influence contraceptive access.
Their earliest lessons about sex, or the lack of them, shaped how adolescents like Karla, Samantha, and Justin understood their health, choices, and access to contraception. In a community where adolescent pregnancy rates remain disproportionately high, understanding the facilitators and barriers to contraceptive access can begin by breaking that (generational) silence, unlearning stigma, and challenging cultural and family expectations that shape their earliest perceptions of sexual health and relationships.